The Polypharmacy Puzzle: Understanding Mechanisms of Drug-Drug Interactions
Every time a patient swallows a tablet, a complex biochemical clock begins to tick. For a drug to exert its therapeutic effect and safely exit the body, it must navigate the intricate pathways of human metabolism. But when a patient is taking multiple medications simultaneously, these pathways can quickly become congested, leading to unexpected therapeutic failures or dangerous toxicities.
Understanding the mechanics of how drugs interact is no longer just a luxury for clinical pharmacologists—it is a daily necessity at the bedside.
How the Body Handles Foreign Substances
Before we can look at what goes wrong, we must look at what happens when things go right. Most medications are inherently lipophilic (fat-soluble)—a property that allows them to be easily absorbed across biological membranes and reach their targets. However, this same trait makes them incredibly difficult for the kidneys to excrete, as lipophilic compounds are simply reabsorbed back into the bloodstream.
To eliminate these substances, the body relies on biotransformation (metabolism), which primarily takes place in the liver. This process converts lipophilic compounds into hydrophilic (water-soluble) metabolites that can be easily cleared through urine or bile.
When analyzing how medications cross paths during this journey, clinical interactions are fundamentally split into two distinct categories:
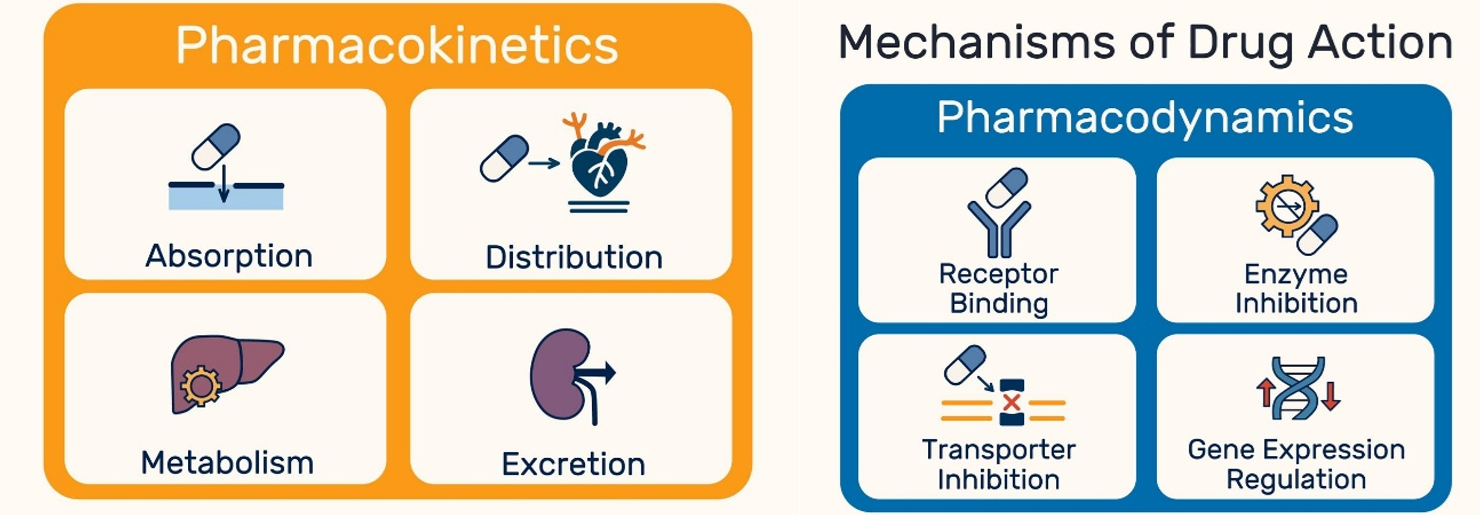
- Pharmacokinetics (PK) – What the body does to the drug: This involves altering the actual concentration of the drug in the bloodstream by changing its Absorption, Distribution, Metabolism, or Excretion (ADME).
- Pharmacodynamics (PD) – What the drug does to the body: This occurs when medications have additive, synergistic, or antagonistic effects directly at the receptor site or target organ—all without changing the actual drug concentrations in the blood.
The Highway of Metabolism: The CYP450 System
The heavy lifting of metabolic biotransformation is performed by a superfamily of heme-containing enzymes known as Cytochrome P450 (CYP450). Embedded within the endoplasmic reticulum of hepatocytes (liver cells) and enterocytes (intestinal cells), these enzymes are responsible for the Phase I metabolism of the vast majority of clinically relevant drugs.
While there are dozens of CYP enzymes, a select few handle the bulk of the clinical workload:
- CYP3A4: The absolute workhorse of the liver, responsible for metabolizing roughly 50% of all prescribed medications.
- CYP2D6: Highly polymorphic (genetically variable), handling many cardiovascular and neuropsychiatric drugs.
- CYP2C9 & CYP2C19: Critical for the clearance of common anticoagulants and the activation of specific cardiovascular therapies.
The Two Core Mechanisms (and the Pro-Drug Trap)
Pharmacokinetic drug-drug interactions (DDIs) typically occur through two primary enzymatic mechanisms. However, their impact depends entirely on whether the drug is administered in an active state or as a pro-drug (which requires enzymatic cleavage to become active):
- Enzyme Inhibition (The Brake): Drug A blocks a CYP enzyme, slowing down the metabolism of Drug B.
- Active Drugs: Causes the drug to accumulate, risking toxicity.
- Pro-drugs: Prevents the drug from activating, causing therapeutic failure.
- Enzyme Induction (The Accelerator): Drug A stimulates the body to synthesize more CYP enzymes, speeding up the metabolism of Drug B.
- Active Drugs: Clears the drug too rapidly, leading to therapeutic failure.
- Pro-drugs: Accelerates activation, potentially spiking active drug levels to toxic thresholds.
Underappreciated Culprits in Daily Practice
While clinicians are well-trained to spot interactions between heavy-hitting prescription drugs, some of the most profound interactions involve over-the-counter supplements and dietary habits that patients frequently omit from their medical histories.
Interacting Agent | Underlying Mechanism | Clinical Consequence |
St. John’s Wort (Hypericum perforatum) | Potent inducer of CYP3A4 and P-glycoprotein (P-gp) efflux transporters. | Drastically reduces concentrations of oral contraceptives (leading to unintended pregnancy), cyclosporine (leading to organ transplant rejection), and direct oral anticoagulants (DOACs). |
Grapefruit Juice | Irreversible inhibitor of intestinal CYP3A4 (lasting up to 72 hours). | Disables first-pass metabolism, significantly spiking serum concentrations of certain statins (e.g., simvastatin) and calcium channel blockers, increasing the risk of rhabdomyolysis or severe hypotension. |
Calcium / Iron / Antacids | Divalent/trivalent cation chelation in the gastrointestinal tract. | Physically binds to fluoroquinolones, thyroid hormones, and integrase inhibitors in the gut, forming an unabsorbable complex that causes complete treatment failure. |
Actionable Recommendations for Safety
For Clinicians
- Review the patient's prescribed frequently: Review medication lists at every transition of care. If a drug no longer has a clear, evidence-based indication, taper it off to minimize the metabolic load on the liver.
- Screen Beyond Prescription Records: Do not just ask what medications a patient takes; explicitly ask about herbal remedies, over-the-counter treatments, and routine dietary habits.
- Utilize Spatial Sequencing Correctly: For physical absorption-based interactions (like chelation), space the interacting agents by at least 2 hours before or 4–6 hours after the supplement. Note: This strategy does not work for enzymatic interactions like grapefruit juice, which require total avoidance due to long-lasting enzyme damage.
For Patients
- Maintain a Master List: Keep an updated digital or physical list of everything you take, including prescription medicines, over-the-counter painkillers, vitamins, and herbal teas.
- The "Single Pharmacy" Rule: Try to fill all prescriptions at the same pharmacy. This allows a single electronic system to cross-reference your entire profile and automatically flag potential discrepancies.
- Consult Before Self-Treating: Always consult a pharmacist or doctor before starting a new over-the-counter supplement, especially if you take medications with a narrow therapeutic window (like blood thinners or anti-seizure medications).
Mastering the Traffic Control of Modern Medicine
Managing polypharmacy is ultimately a balancing act between therapeutic necessity and biological reality. As the clinical landscape shifts toward highly specific, multi-drug regimens to manage complex comorbidities, the potential for biochemical traffic jams will only increase.
By shifting our clinical approach from memorizing static, endless drug lists to fundamentally understanding the underlying pharmacokinetic and pharmacodynamic mechanisms, we transform a complex clinical hazard into a manageable, predictable system. Safe prescribing isn't about avoiding multi-drug therapies altogether; it is about maintaining proactive, mechanistic vigilance at every step of the patient's journey.
Photo credit – POLINA TANKILEVITCH on Pexels: https://www.pexels.com/photo/photo-of-assorted-tablets-3873146/